





放射治疗作为纤维增生性良性病变(如瘢痕疙瘩)的主要及辅助疗法,显著降低局部切除术后高复发风险。文献证实术后辅助放疗可将复发率控制在25%以下(单纯手术复发率>50%)。当前外照射放疗(如浅层X线/电子束)仍是主流方案,其通过抑制成纤维细胞过度增殖实现病灶控制;而新兴证据表明,近距离放疗(Brachytherapy)因精准靶向剂量分布,在降低复发率及保护毗邻组织方面呈现更优疗效趋势。临床决策需综合考量病灶解剖特性(厚度/部位)、医疗资源及成本效益,个体化选择外照射或近距离治疗技术以实现复发控制与安全性平衡。




1.最佳放疗方案:术后24小时内单次10-12Gy照射可实现复发率与不良反应的最优平衡,使用2×9Gy方案可能增加副作用风险且第二剂量必要性存疑;
2.成本效益:浅层X射线(SXRT)单位应用比直线加速器(linac)更具成本效益;







Treatment Efficacy & Protocols
Primary Protocol: Single 10Gy superficial X-ray radiotherapy (SXRT) within 24 hours post-excision achieves a 14.8% 5-year recurrence rate with minimal toxicity.
治疗成效与方案
首次治疗标准: 手术切除后24小时内实施单次10Gy浅层X线放疗(SXRT),5年复发率仅为14.8%,且副作用轻微。
Salvage Protocol: 4Gy quarterly fractions (maximum annual cumulative dose ≤16Gy) yield 0% re-recurrence at 5 years, with mild skin thickening reported in minority cases.
Clinical Breakthrough Significance
Breaks the recurrence cycle via low-dose fractionated radiotherapy after primary treatment failure, achieving secondary radical cure.
No severe complications observed at ≤16Gy annual dose, confirming fractionated therapy safety.
临床突破意义
首创阶梯式剂量框架: 首次治疗失败后,通过低剂量分次放疗成功阻断复发循环,实现二次根治。



Conclusions / 重点总结

同位素疗法临床方案与特性
Sr-90 Fractionated Low-Dose Method 锶-90分次低剂量法
Protocol: 1-2Gy/fraction, weekly ×5 sessions
▸ 方案:1-2Gy/次,每周1次 × 5次(单次10-20分钟)
Enables dynamic observation & customized treatment for irregular lesions
优势:动态观察瘢痕变化,适配不规则厚度病灶(分段定制治疗)
Drawback: High visit frequency compromises compliance
缺陷:患者需频繁复诊(依从性挑战)
Advantage: Minimizes patient trave 优势:减少患者往返次数
Risk: Uncontrolled dosing increases under/over-exposure 风险:剂量难精准控制(欠量/过量风险↑)
Protocol: Continuous application 24-48h 方案:24-48小时持续贴敷
Shares convenience with Method 2, yet identical dosing risks 特性:患者便利性类似单次高剂量法,但存相同剂量控制缺陷。



Conclusions / 重点总结

6 MeV electron beams induce DNA damage in fibroblasts via ionization, suppressing collagen overproduction to prevent recurrence.通过6 MeV电子束电离效应直接损伤成纤维细胞DNA,抑制胶原过度增生,核心目标为预防术后复发(单纯手术复发率>50%)。
Medical linac delivers precise depth control (1.5-2 cm) with <3% dosimetric error, sparing deep tissues.直线加速器提供 1.5-2 cm精准穿透深度(适配绝大多数瘢痕),实现剂量-深度可控性(误差<3%)及深部器官保护。
Requires: ① Conformal lead shielding ② Electron beam compensation ③ Field junction techniques. 需掌握:① 适形铅屏蔽(定制化保护非靶区)② 电子束补偿技术(优化剂量均匀性)③ 野衔接技术。
Treatment window: Initiate within 24-48h post-op治疗时间:术后24-48小时内启动治疗
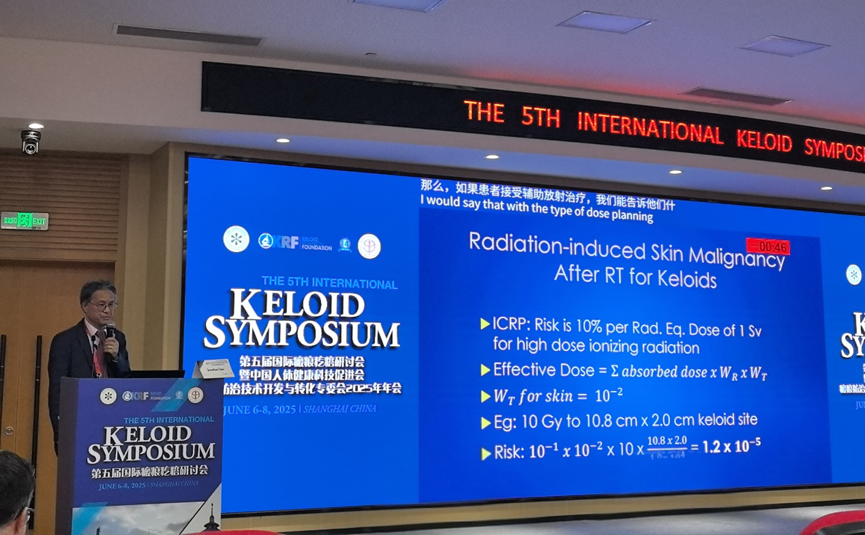
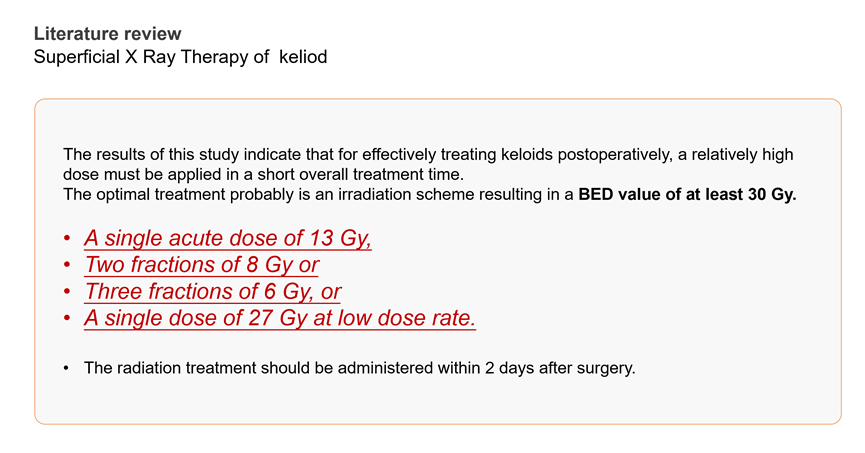
Dosing: BED-guided regimens adjusted by anatomic site. 剂量设计:基于BED公式按解剖位点计算总剂量/分次(如胸骨区需增量10-15%)

众多权威专家强调了瘢痕疙瘩放射治疗的关键价值。当前,放射治疗在瘢痕多学科诊疗体系中占据核心地位,已成为业内共识。未来发展的重点在于:一方面,需推动基层技术的规范化,确保医疗资源相对薄弱地区的基层医疗机构也能精准、安全地应用该技术;另一方面,应针对患者个体差异进一步优化放射剂量,以实现更精准、高效的治疗,最大限度降低副作用,改善患者预后,从而推动瘢痕疙瘩整体治疗水平迈向新高度。
国际权威研究证实,术后辅助放射治疗可将瘢痕疙瘩复发率从单纯手术的>50%显著降至10%以下。当前主流方案聚焦浅层X线放疗(SRT),术后24小时内单次10-12Gy照射可实现复发控制(5年复发率14.8%)与安全性的最佳平衡;复发挽救采用季度分次低剂量(4Gy/次,年累积≤16Gy)可达成二次根治。技术选择需综合考量病灶特性与医疗资源:外照射(电子束/SRT)凭借精准深度控制(1.5-2cm)及铅屏蔽技术保障安全;近距离放疗(如Ir-192)及同位素敷贴(Sr-90/P-32)虽具剂量靶向优势,但面临操作标准化挑战。临床突破在于建立阶梯式剂量框架与BED指导的个体化方案,同时推动基层放疗规范化落地——中国已有50余家医院应用SRT-100系统,为瘢痕疙瘩多学科诊疗体系提供关键技术支撑。
The SRT-100 Superficial Radiotherapy System, produced by US-based Sensus Healthcare, has now been installed and clinically implemented in over 50 hospitals across China.
What is Superficial X-ray Radiotherapy? 什么是浅层X线放射治疗?
Superficial X-ray radiotherapy can be understood as radiotherapy for surface tissues. It uses soft X-rays, which is a type of low-energy radiation therapy. Its tissue penetration is shallow, making it suitable for treating diseases in superficial areas.
浅层X线放射治疗,可以理解为表浅的放疗,用的是软X射线,是一种低能量的放射疗法,其组织穿透力较浅,适合表浅部位的疾病治疗。
What is the difference between Superficial X-ray Radiotherapy and Conventional Tumor Radiotherapy? 浅层X线放射治疗与肿瘤放疗的区别?
Conventional radiotherapy typically refers to treatment with a linear accelerator, or electron beam radiotherapy, which falls under the Department of Radiation Oncology. The radiation emitted by a linear accelerator has high energy, strong penetration, and deep treatment depth, making it suitable for tumors located deeper within the body.
一般所说的放疗,指的是直线加速器,或者叫电子束放疗,属于放疗科。直线加速器输出的射线能量大、穿透力强、照射深度强,用于部位较深的肿瘤放疗。
When used for superficial treatments, it may cause damage to subcutaneous tissues and lead to complications in normal tissues. Superficial X-ray radiotherapy currently employs low-dose radiation with shallow penetration. Before irradiation, the normal skin surrounding the treatment area is protected by lead sheets. The vertical penetration depth does not exceed 2 cm. Its shallow action depth provides better protection for deeper subcutaneous organs.
在用于浅表治疗时,可能会对皮下组织造成损伤,引起正常组织的并发症。浅层X线放射治疗目前采用浅层小剂量的放射治疗,且照射前会将切口周围正常皮肤用铅皮保护起来。照射的垂直深度不超过2cm,作用深度较浅,对皮下深部器官保护比较好。
Mechanism and Principle of Superficial X-ray Radiotherapy?浅层X线放射治疗的机制、原理?
Superficial X-rays can selectively kill and inhibit metabolically active cells and fibrous tissue. At commonly used radiation doses, the radiation causes DNA damage in cells, preventing them from dividing further. Immature fibroblasts, keratinocytes, and tumor cells, among others, are sensitive to X-rays.
浅层X线可以针对性地杀灭和抑制代谢旺盛的细胞和纤维组织。在常用的辐射剂量下,辐射后会造成细胞DNA损伤,细胞不能够再分裂。幼稚的纤维母细胞、角化细胞及肿瘤细胞等都对X射线敏感。
Indications for Superficial X-ray Radiotherapy?浅层X线放射治疗的适应症?
For pathological scars (keloids, hypertrophic scars), postoperative radiotherapy is required to reduce the risk of scar hyperplasia and recurrence.
对于病理性瘢痕(瘢痕疙瘩、增生性瘢痕),术后需要通过放疗来降低瘢痕增生、复发的几率。
Superficial X-ray radiotherapy can also be used to treat:benign dermatological conditions: such as warts, familial benign chronic pemphigus (Hailey-Hailey disease), keratosis follicularis (Darier's disease).Skin tumors: such as cutaneous squamous cell carcinoma, mycosis fungoides.
浅层X线放射治疗还可用于:良性皮肤病,如疣、家族性良性慢性天疱疮、毛囊角化病等。皮肤肿瘤,如皮肤鳞状细胞癌、蕈样肉芽肿等。
最新发布
-

会议通知| 2026上海整形科技周--瘢痕管理班+第8期美容缝合实操班
2026-01-19 16:00
-

手足四肢瘢痕的综合治疗策略:功能康复与美学平衡 | 瘢痕科普
2026-01-12 12:08
-

2026-01-12 12:03
-

2025福建省妇幼保健系统整形美容联盟成立大会暨福建省妇幼保健系统整形美容技术培训班在福州成功举办
2025-12-24 11:09
-

2025-12-15 10:06
热门资讯
-

2024-07-28 23:22
-

2024-07-01 11:55
-

2024-07-01 11:47
-

2024-07-01 11:44
-

2024-07-01 11:31